Endocrine hypertension is a form of hypertension caused by an excess of hormone production by the endocrine glands.
Endocrine hypertension is the most common form of hypertension among those attributable to a specific cause (called secondary hypertension). As in the case of primary hypertension (which have no known cause) they are characterized by blood pressure values above 140/90 mmHg.
Background: In most cases of endocrine hypertension, three classes of hormones produced by the adrenal glands, the glands located just above the kidneys, come into play: cortisol, aldosterone and catecholamines (adrenaline and noradrenaline). These hormones are involved in the regulation of blood pressure and if produced in excessive quantities are associated with hypertension. In most cases, the excess of catecholamines or aldosterone is the consequence of the presence of an adenoma of the adrenal gland, a benign tumor that can affect this gland. In the case of hypertension due to excess cortisol, the disease may be due to a pituitary adenoma which causes hyperstimulation of the adrenal gland (from excess ACTH) or to an adrenal localization adenoma. Finally, it should be remembered that hypothyroidism and hyperthyroidism can be associated with hypertension. Endocrine hypertension due to catecholamines (pheochromocytoma) can be associated with headache, pallor of the face, increased heart rate, sweating and anxiety. In cases of excess cortisol (Cushing’s syndrome), hypertension is associated with clinical manifestations such as central obesity, the presence (in women) of hirsutism, acne and menstrual cycle irregularities, osteoporosis and even severe alterations in blood sugar. . Finally, in the case of excess aldosterone, hypertension is not associated with specific symptoms except, in some cases, with the reduction of potassium levels and the clinical manifestations associated with this reduction
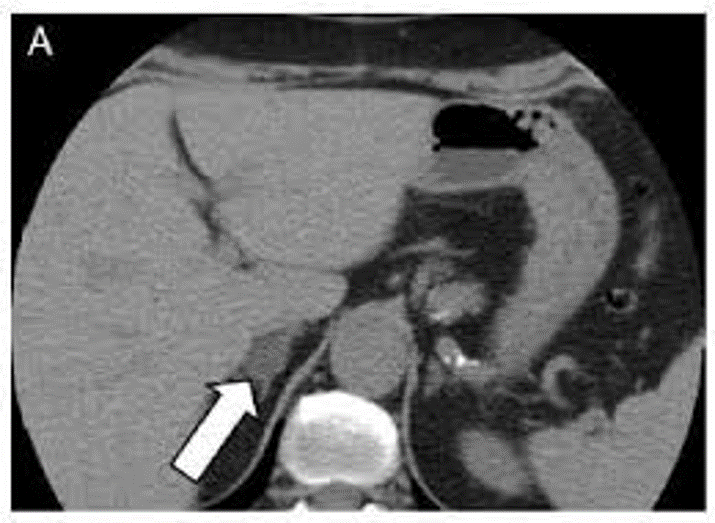
Case Report: 80 year old woman came to the internal medicine ambulatory for bad hypertension (HY) control: two recent accesses in first aid (FA) for hypertensive crisis with values of 205/100 mmHg resolved with clonidine and furosemide. History of ischemic heart disease, diabetes mellitus, dyslipidemia, and HY from 6 years treated with ramipril and amlodipine with good control. Routine exams were normal. We dimetted patient increasing ramipril and adding calcium antagonist. Ten days later she came back to FA for a new episode of severe hypertension (180/100 mmHg). We found: hypokalemia (2.8 mmol/l) and no good glucose control (Hbglicata 8.9%). We decided to suspend ramipril and added clonidine (TTS2) and amlodipine. Urinary electrolytes 24 hours, aldosterone and renin in plasma: normal Kaliuria, high aldosteronemia both in clino and ortho statism, reninemia normal and relationship aldosterone/renin was high. She underwent abdomen functional magnetic resonance magnetic confirmed adrenal 28mm nodule in the posterior region of the right adrenal gland. She began therapy canrenone100 mg and clonitinaTTS2. She had a good response.
Conclusions: the renovascular hypertension is common in the elderly, the endocrine etiology is common among 40-50 anni. We cannot exclude secondary causes of hypertension in the elderly.
Authors: O. Grassi, A. Aceranti, G. Alessandro, R. Cattaneo, F. Deantoni, R. Padalino, E. Pagliaro, C. Ternavasio, T. Candiani, S. Vernocchi
Published: Italian Journal of Medicine 2016
Presented: Poster FDI6430-16 at the FADOI National Congress of Medicine 2016